What Is Libido in Men? A Comprehensive Guide to Sexual Desire, Hormones, and Psychology
Libido in men is defined as the overall sexual drive or motivational state to seek sexual activity, governed by a complex interplay of hormonal signals, neurotransmitter activity, and psychological well-being [L1, L4].
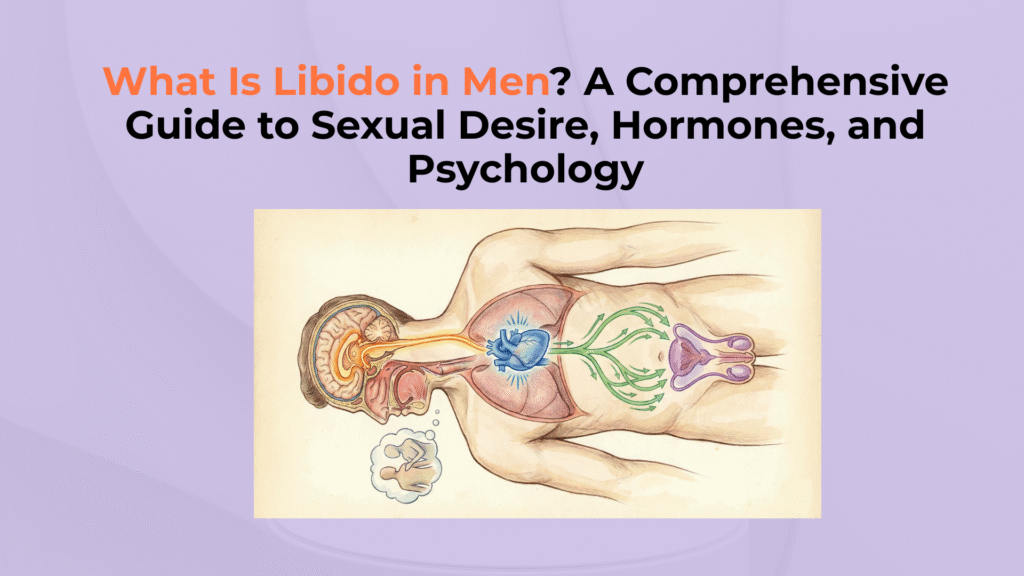
This guide explores the biological “fuel” (Testosterone), the neural “spark” (Dopamine), and the psychological context required to maintain a healthy drive.
Important Medical Disclaimer
This guide is for educational purposes only. Persistent loss of sexual desire can be a symptom of underlying endocrine or cardiovascular conditions. Consult a healthcare provider for diagnosis.
Male Libido: At a Glance
- ▸ What is it? The “Engine” (Desire), not the “Wheels” (Erection).
- ▸ Primary Driver: Testosterone (Hormonal Fuel).
- ▸ Primary Inhibitor: Stress/Cortisol (The “Brake”).
- ▸ Key Distinction: You can have low libido with normal erections, and vice versa.
What Is the Biological and Psychological Definition of Libido?
The biological and psychological definition of libido frames sexual desire as a Bio-Psycho-Social phenomenon, integrating physiological readiness with mental motivation [L1].
Defining Libido (The Bio-Psycho-Social Entity)
Libido is clinically defined as a person’s overall sexual drive, functioning not as a simple “on/off” switch but as a dynamic integration of hormones, brain chemistry, and emotional state [L1].
Crucially, this biological drive must be distinguished from Erectile Function (mechanical ability) and Fertility (reproductive ability).
According to Levine, hormonal signals interact with psychological context to produce the conscious state of sexual desire [L3].
The Premise: The “Need” vs. “Want” Dynamic
The premise of libido operates on a “Need vs. Want” dynamic, functioning primarily as a motivational state that drives behavior. It is the neural translation of biological fitness into a conscious urge.
The biological drive for reproduction combines with psychological stimuli, resulting in a conscious state of sexual desire [L4].
How Do Hormones and Brain Chemistry Govern Male Libido?
Hormones and brain chemistry govern male libido through the primary androgenic “fuel” of Testosterone and the neurochemical “spark” of Dopamine [L2, L4].
The Role of Testosterone (The Fuel)
Testosterone is a primary driver of male sexual desire; low levels are associated with reduced libido, and clinical diagnosis requires symptoms plus consistently low measured testosterone [L2].
It acts at central nervous system levels to modulate desire. Adequate testosterone levels activate neural pathways of desire, ensuring a functional baseline libido [L7].
The Role of Neurotransmitters (The Spark)
The role of neurotransmitters involves Dopamine acting as the excitatory “spark” of reward, while Serotonin and Prolactin often function as inhibitory “brakes” [L4].
High dopamine drives pursuit and motivation, whereas high serotonin can suppress drive. Dopamine release in the brain triggers the motivation to seek sexual reward, leading to the initiation of arousal.
What Are the Primary Causes of Low Libido (HSDD) in Men?
The primary causes of Low Libido, clinically termed Male Hypoactive Sexual Desire Disorder (MHSDD), generally fall into two categories: Physiological deficits and Psychological inhibitors [L6].
Physiological Causes: Hormones and Health
Physiological causes center on Hypogonadism (low testosterone) and systemic health factors that impair metabolic function [L2].
Chronic conditions like diabetes, obesity, and cardiovascular disease provide the context for sexual symptoms.
Medications like SSRIs alter neurochemical balance, often contributing to a reduction in sexual drive [L4].
Psychological Causes: The Mental “Brake”
Psychological causes act as a mental “brake,” primarily driven by chronic stress, cortisol elevation, and mental health conditions like depression.
Chronic stress floods the body with Cortisol, which can be antagonistic to Testosterone in stress contexts. High cortisol levels inhibit the production and action of testosterone, causing a rapid decline in sexual interest [L5].
How Does Libido Differ from Erectile Function?
Libido differs from Erectile Function as the distinction between the psychological “Engine” (Desire) and the physical “Wheels” (Mechanics) [L3].
Desire vs. Mechanics (The Engine vs. The Wheels)
Libido represents the mental urge or hunger for sex (The Engine), whereas Erectile Function represents the vascular and neural ability to fill the penis with blood (The Wheels).
One can exist without the other; men with ED often still have high desire. Strong libido provides the mental signal for arousal, but cannot overcome a mechanical vascular failure [L3].
[Checklist] Auditing Your Libido and Sexual Health
Use this functional and health audit checklist to evaluate the potential drivers of your current libido status.
Functional and Health Audit
- Hormone Check: Have you had Total and Free Testosterone tested? [L2].
- Medication Audit: Are you taking SSRIs or other meds affecting neurochemistry?
- Stress Levels: Is chronic stress elevating Cortisol? [L5].
- Sleep Quality: Getting 7-8 hours for REM-based Testosterone production?
- Diagnosis: Has distress lasted >6 months (MHSDD criteria)? [L6].
- ⚠ Safety Rule: Low libido is often a symptom of underlying health issues; consult a provider.
Conclusion
In conclusion, male libido is a multifaceted bio-psycho-social state driven by testosterone and dopamine, yet easily disrupted by stress, systemic health, and medication. Sustainable sexual health requires addressing both the engine (libido) and the mechanics (erection), recognizing that desire originates in the brain but relies on the body for execution.
Clinical References
- [L1] Levine SB. “Reexploring the concept of sexual desire.” PubMed
- [L2] AUA. “Evaluation and Management of Testosterone Deficiency” AUA Guidelines
- [L3] AUA. “Erectile Dysfunction: AUA Guideline” AUA Guidelines
- [L4] Pfaus JG. “Pathways of sexual desire.” J Sex Med
- [L5] Hamilton LD, et al. “Cortisol, sexual arousal, and affect…” PMC
- [L6] EAU Guidelines. “Male Hypoactive Sexual Desire Disorder.” EAU
- [L7] Corona G. “The role of testosterone in male sexual function.” PMC



4 Responses