What Are the Main Arteries That Supply Blood to the Penis?
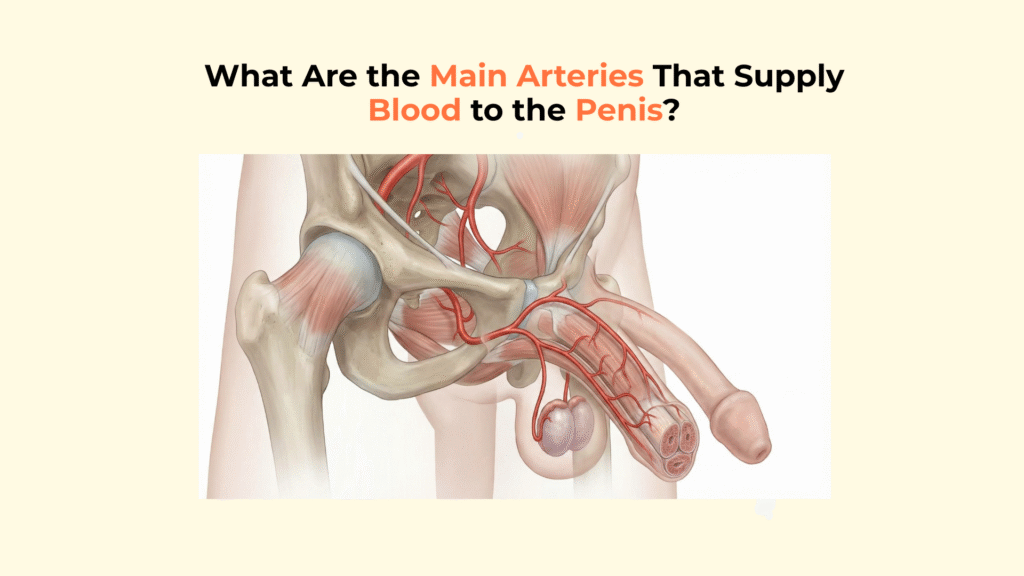
The main arteries supplying blood to the penis are the three terminal branches of the internal pudendal artery: the bulbourethral artery, the dorsal artery, and the cavernosal (deep) artery, each serving a specific physiological role in nutrition or erection.
While all three vessels transport oxygenated blood to the organ, they perform drastically different functions. One branch is responsible for keeping the skin alive, another maintains the health of the urethra, and the third acts as the high-pressure line that physically drives the hydraulic expansion of an erection.
This guide provides a detailed anatomical map of the penile arterial system, tracing the flow from the pelvis to the specific branches and explaining the micro-vascular mechanisms that regulate inflow.
Important Medical Disclaimer: This information is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Consult with a qualified healthcare provider regarding any medical condition or concerns about your health.
Key Vascular Facts: Penile Arteries
- The Source: All penile blood supply originates from the Internal Pudendal Artery.
- Bulbourethral: Supplies the corpus spongiosum and glans (nutritional/metabolic).
- Dorsal Artery: Runs along the top of the penis; supplies skin, fascia, and the glans.
- Cavernosal: Also called the Deep Artery. Runs inside the corpora cavernosa; it is the primary “engine” of erection.
- Micro-Regulators: The Helicine Arteries are tiny, corkscrew-shaped branches that act as the final valves to control blood flow.
What Is the Origin of the Main Arteries Supplying the Penis?
The arterial supply to the penis originates from the anterior division of the Internal Iliac Artery, which gives rise to the Internal Pudendal Artery, the primary vessel for the entire perineal region. This vascular path ensures that blood flow is channeled securely from the deep pelvis before reaching external structures.
The “Internal Pudendal” Pipeline
The “Internal Pudendal Pipeline” describes the specific route the artery takes as it travels out of the pelvis, through the gluteal region, and into the perineum via Alcock’s canal.
Upon exiting the canal and reaching the perineum, the vessel transitions into the Common Penile Artery. It then terminates by trifurcating (splitting into three) into the specific penile branches that service the organ. This trifurcation is the critical transition point where general pelvic blood flow becomes specialized penile circulation.
Source: StatPearls – Internal Pudendal Artery
What Are the Three Terminal Branches of the Penile Artery?
The Common Penile Artery divides into three distinct terminal branches: the Bulbourethral Artery, the Dorsal Artery, and the Cavernosal (Deep) Artery, each targeting a specific tissue compartment.
The arterial walls themselves are anchored by surrounding structures, including the supportive layers of the tunica albuginea . This fibrous envelope compresses venous channels against the sub-tunical plane, creating the pressure trap necessary for a rigid erection. Even minor asymmetry in this layer can produce uneven arterial expansion.
The Bulbourethral Artery (The “Primer”)
The Bulbourethral Artery enters the bulb of the penis to supply oxygenated blood to the corpus spongiosum and the urethra. Its primary role is metabolic rather than mechanical. It ensures the urethra remains viable and contributes to the engorgement of the glans (head) during arousal. Without this steady supply, the tissues surrounding the urinary tract would lack necessary oxygenation.
The Dorsal Artery (The “Sustainer”)
The Dorsal Artery runs along the top (dorsum) of the penis, positioned between the dorsal nerve and the deep dorsal vein, superficial to the tunica albuginea.
This artery targets the outer layers. It provides nutritional blood flow to the shaft skin and engorgement to the head, but contributes minimally to shaft rigidity. It is the vessel responsible for maintaining the health of the penile fascia and the integumentary system of the penis.
On the surface, arterial responsiveness can be influenced by the configuration of the glans penis , which receives blood via the dorsal network rather than the cavernosal system. In contrast, the proximal inflow is stabilized by the musculature around the pelvic base, especially the perineal base muscles , which enhance intracavernosal pressure through rhythmic contraction.
Pathologies add an important layer of complexity. In Peyronie’s disease , plaque formation along the tunica disrupts normal arterial curvature and can create areas of restricted inflow. Similarly, early stages of arteriogenic erectile dysfunction often manifest as reduced responsiveness in the penile arterial tree , long before total occlusion appears on imaging.
The Cavernosal (Deep) Artery (The “Engine”)
The Cavernosal Artery, also known as the Deep Artery, pierces the crus and runs through the center of each Corpus Cavernosum.
This vessel targets the erectile tissue (sinusoids). Anatomically and functionally, the deep cavernosal artery serves as the primary inflow channel during arousal, driving the hydraulic pressure needed for erection. It is the central component of the erectile mechanism.
The hemodynamic behavior of the penile arteries depends heavily on the integrity of the corpora cavernosa , since these paired chambers receive the majority of inflow during tumescence. Any disruption to their smooth muscle or endothelial lining alters expansion capacity and arterial responsiveness.
If fibrosis develops in the cavernosal tissue, arterial inflow may be preserved but expansion becomes impaired. The reduced compliance limits how effectively blood pressure can build within the cavernosal drainage system , producing a condition clinically similar to venous leak despite normal upstream arterial supply.
How Do the Helicine Arteries Regulate Flow?
The Helicine Arteries regulate flow by acting as microscopic valves; they are tiny, coiled branches of the Cavernosal Artery that open directly into the lacunar spaces (sinusoids).
The initial surge of blood enters through branches of the internal pudendal system, especially the helicine arteries . These microscopic vessels straighten under parasympathetic signaling, allowing unrestricted flow toward the deep cavernosal vascular pathway , which transitions the penis from a low-pressure to a high-pressure system within seconds.
The “Valve” Mechanism
The “Valve” mechanism of the Helicine Arteries is controlled by the autonomic nervous system, determining whether the penis is flaccid or erect.
The term “helicine” refers to their spiral or corkscrew-shaped structure. In the flaccid state, these arteries are coiled and constricted (high sympathetic tone), limiting inflow to a nutritional baseline. During the erect state, they uncoil and dilate (driven by parasympathetic release of Nitric Oxide), dumping blood directly into the lacunar spaces. This rapid dilation allows arterial blood to fill the spongy tissue, expanding the penis.
The neural drive controlling these arterial transitions arises from both somatic and autonomic pathways. Sensory feedback from the dorsal nerve of the penis integrates with parasympathetic fibers that coordinate vasodilation and sinusoidal filling. Any impairment in these pathways affects arterial tone and cavernosal expansion.
Source: NCBI – Physiology of Erection
These relationships demonstrate that penile hemodynamics depend on the coordinated function of the spongiosal-urethral complex , the cavernosal bodies, the tunical envelope, and the neuromuscular inputs sustaining pressure. When any part of this system becomes compromised — anatomically or pathologically — the arterial waveform reflects the underlying disorder.
Comparative Matrix: The 3 Terminal Penile Arteries
This table provides a direct comparison of the three terminal branches of the penile artery, detailing their location and primary physiological function.
| Artery Name | Location | Primary Function |
|---|---|---|
| Bulbourethral Artery | Bulb / Corpus Spongiosum | Urethral health; Glans engorgement |
| Dorsal Artery | Top of shaft (Sub-Buck’s Fascia) | Skin nutrition; Glans engorgement |
| Cavernosal (Deep) Artery | Center of Corpora Cavernosa | Shaft Rigidity; The “Engine” of erection |
☑ Identifying the Main Penile Arteries
Use this checklist to verify your understanding of the penile arterial system.
Glossary of Anatomical Terms
To ensure full clarity, this glossary defines the key anatomical terms used throughout this guide.
| Internal Pudendal Artery | The main artery of the perineum that supplies blood to the external genitalia. |
| Cavernosal Artery | The deep artery running through the center of the corpora cavernosa, responsible for erection. |
| Dorsal Artery | The artery running along the top of the penis, supplying the skin and glans. |
| Helicine Arteries | Small, corkscrew-shaped arteries that branch off the cavernosal artery and open into the erectile tissue. |
| Alcock’s Canal | An anatomical tunnel in the pelvis through which the internal pudendal artery and nerve pass. |
Frequently Asked Questions: Penile Arteries
Which artery is most responsible for erectile hardness?
The Cavernosal (Deep) Artery is the primary driver of rigidity. It runs directly through the erectile tissue and delivers the high-pressure blood flow required to expand the corpora cavernosa.
Can atherosclerosis in these arteries cause Erectile Dysfunction (ED)?
Yes. Because the penile arteries are smaller than the coronary arteries (heart), they can be blocked by plaque earlier. This condition, known as vasculogenic ED, restricts the inflow necessary to achieve or maintain an erection.
What is the difference between the Dorsal Artery and the Deep Dorsal Vein?
The Dorsal Artery brings oxygenated blood into the glans and skin (high pressure). The Deep Dorsal Vein drains deoxygenated blood out of the glans (low pressure). They run parallel to each other along the top of the shaft.
Do the three arterial branches communicate with each other?
Yes, there are often anastomoses (connections) between the dorsal and cavernosal arteries, particularly near the glans. However, their primary physiological roles—nutrition for the dorsal, mechanical expansion for the deep—remain distinct.
Conclusion
In conclusion, the arterial supply to the penis is a sophisticated vascular network derived from the internal pudendal artery, with specific branches dedicated to maintaining tissue health and others engineered specifically to drive the high-pressure hydraulics of an erection.
We have reviewed the “Big 3” branches: the bulbourethral, the dorsal, and the deep cavernosal arteries. While the Deep Artery acts as the engine for rigidity, the Dorsal Artery functions as the vital life-support system for the skin and glans. At Factbasedurology, we believe that understanding your vascular health is the key to preserving it. From the deep pelvic vessels to the tiny helicine coils, this system is a masterpiece of biological engineering.
One Response