Libido Hub
How Does Chronic Stress Blunt Male Libido?
Understanding HPA-axis activation, cortisol, fatigue, mood strain, and sexual motivation
Quick Answer
Chronic stress can reduce male libido by keeping the body in a prolonged threat-response state. That state may alter HPA-axis signaling, raise or flatten cortisol rhythms, interfere with reproductive hormone signaling, worsen sleep, increase fatigue, and make sexual interest feel less biologically or emotionally available. The effect is usually multifactorial, not simply “high cortisol equals low testosterone.”
Medical Safety Notice
This article is for education only and does not diagnose low testosterone, depression, anxiety, erectile dysfunction, or another medical condition. Persistent low libido, erectile difficulty, severe fatigue, chest pain, unexplained weight change, suicidal thoughts, or relationship-distressing symptoms should be discussed with a qualified clinician.
Male libido is not controlled by one hormone alone. Desire depends on reproductive hormones, sleep quality, emotional safety, relationship context, energy, mental attention, and reward signaling in the brain.
Chronic stress matters because it can occupy several of those systems at the same time. It can keep the stress-response system active, disturb sleep, increase rumination, and make intimacy feel like another demand rather than a source of connection. When that pattern continues for weeks or months, libido can drop even when testosterone is normal.
The safest way to understand cortisol and libido is as a stress-system relationship, not a single-cause explanation. Cortisol is useful and necessary; the problem is prolonged dysregulation, poor recovery, and the combined effect of stress, fatigue, sleep disruption, mood strain, and reproductive signaling.
Chronic Stress vs. Acute Stress: Why Duration Matters for Libido
Acute stress is short-term. It prepares the body for action, then should settle. Chronic stress is different: the stressor, worry, workload, conflict, or threat perception continues long enough that recovery becomes incomplete. Medical references describe chronic stress as prolonged exposure that can produce cumulative physical and psychological effects.[5]
The acute stress response: useful in the short term
Short-term stress can increase alertness, mobilize energy, and help the body respond to a specific challenge. When the stressor passes, the nervous system and endocrine system should move back toward baseline. This is why one stressful day does not automatically mean a man has a libido disorder.
The chronic stress response: recovery never fully arrives
Chronic stress becomes more relevant to libido when pressure continues and recovery habits are weak. The body may stay in a high-alert state, sleep becomes lighter, irritability rises, and sexual attention becomes harder to access. This is the practical reason many men notice desire returning after stress management improves, even without sexual medication.
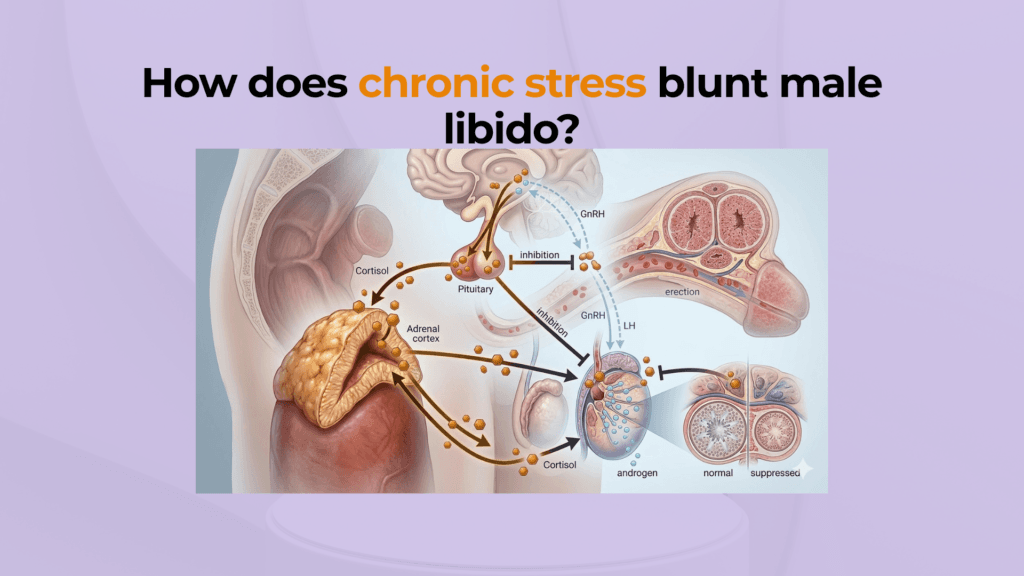
The Cortisol Cascade: How Prolonged Stress Can Suppress Desire
The endocrine stress system can interact with the reproductive system. NCBI’s endocrine physiology review notes that HPA-axis activation can suppress reproductive function, and in men these effects can be associated with decreased libido and fertility changes.[1] That does not mean every stressed man has low testosterone; it means stress is one possible contributor that should be interpreted alongside sleep, mood, medication, medical history, and relationship context.
Cortisol can affect testosterone biology, but the wording must stay precise
Experimental and review literature suggests stress-related glucocorticoids can inhibit testosterone-biosynthetic enzyme activity in Leydig cells, reducing testosterone secretion under some conditions.[2] A safer clinical wording is: chronic stress may contribute to testosterone-related changes in some men. Avoid saying cortisol always “steals” cholesterol or directly blocks testosterone receptors in every case.
Low testosterone is not diagnosed from libido symptoms alone
Low desire, fatigue, and poor mood can occur with stress, poor sleep, depression, medication side effects, relationship strain, and medical disease. The Endocrine Society recommends diagnosing hypogonadism only when symptoms and signs are present together with unequivocally and consistently low testosterone levels.[3] If symptoms persist, testosterone testing should be interpreted with professional guidance rather than used as a stand-alone explanation.
Beyond Hormones: Why Stress Can Make Desire Feel Unavailable
Stress affects the body, but it also affects attention. The American Psychological Association notes that stress, distraction, and fatigue may reduce sexual desire.[4] In real life, this means a man may still love his partner and still feel attraction, but his mind is too overloaded to shift into intimacy.
Mental exhaustion and burnout can blunt sexual initiation
Burnout reduces the spare energy needed for affection, initiation, and presence. If pleasure-seeking begins to feel like work, a man may avoid sex not because attraction has disappeared, but because his system is conserving energy. A structured burnout recovery plan should address sleep, workload, boundaries, movement, and psychological support.
Dopamine and reward signaling should be described carefully
Sexual desire involves reward and motivation circuits, including dopamine-related pathways. But it is too strong to claim that cortisol simply “competes with dopamine transporters” in ordinary stress-related libido loss. A safer explanation is that chronic stress can reduce reward sensitivity, increase rumination, and make sexual cues less motivating. Read more on dopamine and libido for the broader motivation pathway.
How Can You Tell If Stress Is Contributing to Low Libido?
Stress-related low libido is more likely when desire drops during a clear pressure period and appears alongside fatigue, irritability, poor sleep, rumination, low mood, or reduced emotional connection. It is less clear when libido is low without any obvious stress pattern, when erectile function changes suddenly, or when other medical symptoms appear.
Signs stress may be involved
- Low desire appears during prolonged work, financial, family, or relationship pressure.
- Sex feels mentally demanding rather than emotionally connecting.
- Sleep quality, patience, and mood declined before libido declined.
- Desire improves during rest periods, vacations, or lower-pressure weeks.
Signs to assess medically
- Low libido persists for months despite improved sleep and stress management.
- There is persistent erectile difficulty, loss of morning erections, infertility concern, or testicular symptoms.
- There is severe depression, anxiety, panic, substance use, or medication-related change.
- There is unexplained weight change, chest pain, severe fatigue, or other systemic symptoms.
Differentiate low desire from erectile dysfunction
Low libido is mainly a problem of wanting. Erectile dysfunction is mainly a problem of getting or keeping an erection firm enough for sex. They can overlap, but they are not identical. Understanding ED vs low libido helps decide whether the next step is stress reduction, mental health support, testosterone evaluation, cardiovascular screening, or a combined approach.
When Does Stress-Induced Low Libido Require Professional Attention?
Seek professional care when low libido persists, causes distress, damages the relationship, appears with erectile dysfunction, or comes with red flags. Psychiatric disorders and sexual dysfunction can overlap, and anxiety or depression may need direct treatment rather than being treated as a minor stress problem.[6]
| Situation | Usually reasonable to start with self-care | Seek professional review |
|---|---|---|
| Duration | Short-term drop during a clear pressure period | Persistent low desire for several months or worsening pattern |
| Severity | Mild decline with preserved relationship connection | Major distress, avoidance, conflict, or loss of quality of life |
| Associated symptoms | Fatigue and worry that improve with rest | Depression, panic, erectile dysfunction, chest pain, unexplained weight change, infertility concern, or suicidal thoughts |
| Hormone concern | No clear hypogonadal symptoms beyond temporary low desire | Persistent low libido plus loss of morning erections, infertility, low energy, or other signs needing proper lab interpretation |
Stress management is first-line when the pattern is clearly situational
When libido drops during a clear stress period, start by improving recovery: sleep regularity, exercise that does not become overtraining, reduced alcohol, fewer late-night screens, workload boundaries, and partner communication. A practical stress management plan is often more useful than chasing a single supplement or hormone explanation.
Professional assessment is needed when the pattern does not resolve
If libido remains low after stress and sleep improve, evaluation can check for depression, anxiety, medication side effects, thyroid disease, metabolic disease, sleep apnea, hypogonadism, and relationship factors. The goal is not to label the problem as “all in your head” or “all hormones.” The goal is to identify the strongest driver and treat it correctly.
Practical Recovery Plan: What to Fix First
- Track the pattern for 2–4 weeks. Note stress level, sleep time, morning energy, libido, mood, alcohol, exercise, and relationship tension.
- Fix sleep and recovery first. Chronic stress and poor sleep reinforce each other. A consistent wake time, morning light, and lower late-night stimulation can reduce the all-day threat state.
- Lower cognitive load before intimacy. Create a transition ritual: shower, walk, prayer/meditation, breathing, or no-phone time before connecting with your partner.
- Discuss pressure without blaming desire. Say, “My stress is affecting my energy and attention,” instead of framing the issue as rejection.
- Escalate when symptoms persist. If low libido remains despite recovery habits, ask a clinician about mental health, medication effects, cardiometabolic risk, sleep apnea, and hormone testing.
Bottom Line
Chronic stress can blunt male libido, but the mechanism is usually layered: HPA-axis activation, cortisol rhythm changes, possible testosterone effects, poor sleep, fatigue, low mood, rumination, and relationship strain. The strongest fix is not to treat libido as a separate isolated symptom. Treat the recovery system, then evaluate hormones or mental health when symptoms persist.
References & Evidence Sources
- Tsigos C, Kyrou I, Kassi E, Chrousos GP. Stress: Endocrine Physiology and Pathophysiology. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK278995/
- Hardy MP, Gao HB, Dong Q, et al. Stress hormone and male reproductive function. PubMed. https://pubmed.ncbi.nlm.nih.gov/16079965/
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. https://www.endocrine.org/clinical-practice-guidelines/testosterone-therapy
- American Psychological Association. Stress effects on the body. https://www.apa.org/topics/stress/body
- Chu B, Marwaha K, Sanvictores T, et al. Physiology, Stress Reaction. StatPearls / NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK541120/
- Herder T, et al. Sexual dysfunction related to psychiatric disorders. PubMed. https://pubmed.ncbi.nlm.nih.gov/37279603/


