What Is the Difference Between Somatic and Autonomic Innervation of the Penis?
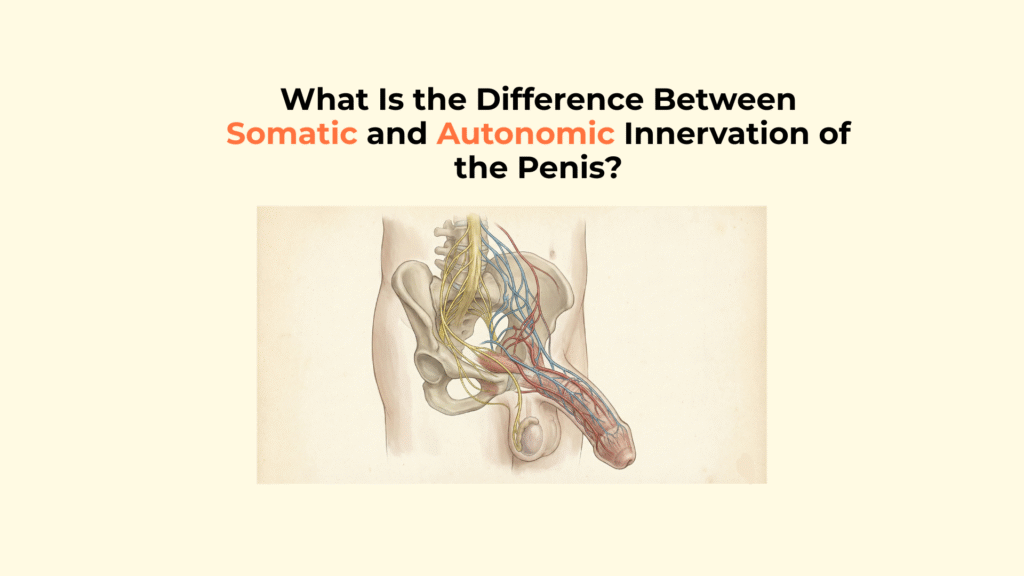
The difference between somatic and autonomic innervation of the penis is their fundamental role: the somatic system (Dorsal Nerve) handles conscious sensation and motor function (ejaculation), while the autonomic system (Cavernous Nerves) handles involuntary physiological control, specifically blood flow for erection.
The penis is a biological machine with two completely separate electrical circuits—one for feeling and one for plumbing—and understanding this division is key to understanding sexual health. This guide details the functional and anatomical distinction between the somatic and autonomic systems, explaining how they cooperate to enable sensation, rigidity, and ejaculation.
Important Medical Disclaimer
This information is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Consult with a qualified healthcare provider regarding any sudden changes in sensation or erectile function.
Key Neurological Differences
- Somatic Role: Governs sensation (feeling, via Dorsal Nerve) and voluntary actions (ejaculation force).
- Autonomic Role: Governs involuntary functions, primarily blood flow control (erection).
- The Nerves: Dorsal Nerve is Somatic. Cavernous Nerves are Autonomic.
- The Mechanism: Autonomic nerves modulate the smooth muscle tone of arteries to control vasodilation (erection) and vasoconstriction (flaccidity).
- Clinical Separation: Damage to the Cavernous Nerves (e.g., prostatectomy) causes loss of erection but spares sensation.
What Is the Functional Distinction Between Somatic and Autonomic Innervation?
The functional distinction between somatic and autonomic innervation is control: somatic is the conscious control system (you decide to move), and autonomic is the unconscious physiological control system (your body breathes without your input).
Somatic (The Conscious System)
The Somatic System provides the sensory input (Afferent/Inbound) and voluntary motor control (Efferent/Outbound) for the penis. It governs feeling (touch, temperature, pain) and the muscular contractions (e.g., ejaculation). This answers the question: “What is the penis feeling and doing under conscious control?”
Autonomic (The Unconscious System)
The Autonomic System controls the internal, involuntary physiological state of the penis, specifically the blood vessels and smooth muscle. It governs vasodilation (erection) and vasoconstriction (detumescence). The Autonomic System modulates the smooth muscle tone of arteries and sinusoids, directly controlling blood flow and the state of erection.
How Does Somatic Innervation (The Dorsal Nerve) Contribute to Penile Function?
Somatic innervation contributes to penile function by providing the sensory trigger for the erection reflex and the motor force required for ejaculation.
Along the shaft, the nerve remains shielded beneath the deep fibrous sheath known as Buck’s fascia, which protects the entire neurovascular bundle from superficial compression. Within this protected compartment, the dorsal nerve travels alongside the deep dorsal vein of the penis and the paired dorsal arteries.
Sensory Input (The Erection Trigger)
The Dorsal Nerve of the Penis (branch of the Pudendal Nerve) transmits high-resolution tactile information from the glans to the spinal cord. The final sensory termination of the dorsal nerve occurs within the glans penis, where dense mechanoreceptor concentration converts tactile deformation into high-fidelity afferent neural signals. This sensory input is essential for initiating the spinal reflex arc that immediately triggers the autonomic (erectile) response.
Motor Output (The Ejaculatory Drive)
The Perineal Branches of the Pudendal Nerve provide voluntary motor control to the Bulbospongiosus and Ischiocavernosus muscles. These muscles contract forcefully, driven by the somatic system, to expel semen and enhance rigidity during orgasm.
How Does Autonomic Innervation (The Cavernous Nerves) Control Penile Hemodynamics?
Autonomic innervation controls penile hemodynamics by using the Cavernous Nerves to release opposing neurotransmitters that either cause vessel widening (erection) or vessel tightening (flaccidity). While the dorsal nerve transmits conscious sensory input, erection itself is governed by the opposing autonomic forces described in autonomic blood flow regulation, illustrating the somatic–autonomic reflex loop.
Parasympathetic Role (The Erection Inducer)
The Parasympathetic Cavernous Nerves (S2-S4) release Nitric Oxide (NO), which causes smooth muscle relaxation, initiating vasodilation (inflow) and venous compression (trap).
Once parasympathetic activation dominates, vascular expansion occurs within the corpora cavernosa, converting sensory excitation into functional penile rigidity. The stability of this rigidity further depends on compression of the cavernosal venous drainage system, preventing premature outflow during peak tumescence. This pressurized state is mechanically preserved by the tensile resistance of the tunica albuginea, which functions as the final structural containment layer.
Sympathetic Role (The Detumescence Inducer)
The Sympathetic Cavernous Nerves (T11-L2) release Norepinephrine, which causes smooth muscle contraction. This leads to arterial vasoconstriction (inflow reduction) and maintenance of the flaccid state.
Comparative Matrix: Somatic vs. Autonomic Innervation
This table provides a direct comparison of the functional and anatomical roles of the somatic and autonomic systems in penile function.
| System | Role | Main Nerve | Primary Target Tissue |
|---|---|---|---|
| Somatic | Conscious Sensation/Motor | Dorsal Nerve/Pudendal | Skin/Glans/Muscles |
| Autonomic – Parasympathetic | Erection/Vasodilation | Cavernous Nerves | Arterial/Smooth Muscle |
| Autonomic – Sympathetic | Flaccidity/Vasoconstriction | Cavernous Nerves | Arterial/Smooth Muscle |
What Are the Clinical Implications of Separating the Two Systems?
The anatomical separation of the somatic and autonomic systems has profound clinical implications, as injury or surgery can selectively damage one system while sparing the other.
Trauma and Selective Loss of Function
Damage can cause a “selective loss of function” where a patient may retain the ability to feel but lose the ability to have an erection, or vice-versa.
- Scenario 1 (Somatic Loss): Damage to the Pudendal Nerve (e.g., cycling injury) causes loss of sensation (numbness) but may preserve reflex erection (Autonomic nerves are intact).
- Scenario 2 (Autonomic Loss): Damage to the Cavernous Nerves (e.g., prostatectomy) causes loss of the ability to achieve full rigidity (arterial control fails) but preserves sensation (somatic nerves are intact). See nerve-sparing prostatectomy.
Additionally, in fibrotic curvature disorders such as Peyronie’s disease, asymmetrical tensile forces can distort both corporal expansion and sensory nerve trajectory.
Pharmacological Targets
Erectile Dysfunction drugs (PDE5 inhibitors) specifically target the Autonomic/Parasympathetic pathway, amplifying the effects of Nitric Oxide (NO). They have absolutely no effect on the somatic pathway, meaning they can restore blood flow but cannot restore lost sensation due to nerve damage. Reference: PDE5 inhibitors information.
Essential Differences in Penile Innervation Checklist
Use this checklist to review the essential functional distinctions between the two neurological systems.
- Feeling/Movement: Is the Somatic system linked to feeling and ejaculation?
- Blood Flow: Is the Autonomic system linked to blood vessel control (erection)?
- Nerves: Are the Dorsal/Pudendal nerves Somatic? Are the Cavernous nerves Autonomic?
- Antagonism: Is the Sympathetic (Flaccid) vs. Parasympathetic (Erect) balance clear?
- Clinical Separation: Is it understood that damage can selectively affect one system while sparing the other?
Glossary of Neurological Terms
To ensure full clarity, this glossary defines the key neurological terms used throughout this guide.
| Term | Definition |
|---|---|
| Somatic Nervous System | The part of the nervous system responsible for conscious control, movement, and external sensation. |
| Autonomic Nervous System | The part of the nervous system responsible for involuntary functions, like blood flow, heart rate, and digestion. |
| Dorsal Nerve of the Penis | The somatic nerve responsible for transmitting touch and pain sensation from the glans penis. |
| Cavernous Nerves | The autonomic nerves that carry the signals for erection (NO) and flaccidity (Norepinephrine). |
| Nitric Oxide (NO) | The primary neurotransmitter released by parasympathetic nerves to induce smooth muscle relaxation and erection. |
| Spinal Reflex Arc | A neural pathway that controls a reflex action (like reflex erection) directly through the spinal cord. |
Conclusion
In conclusion, the fundamental difference between somatic and autonomic innervation is the neurological separation between feeling and function, a sophisticated design that allows the body to both enjoy and execute sexual activity.
The somatic system allows you to feel the interaction, while the autonomic system quietly manages the hydraulic pressure required to maintain it. This distinction explains why medical conditions can damage one while sparing the other—creating unique challenges in urology.
At Factbasedurology, we believe that understanding the complexity of your neural wiring is the first step to preserving your sexual health. The precise interaction between the ‘feeling’ nerves and the ‘plumbing’ nerves is the physiological secret to sexual function.