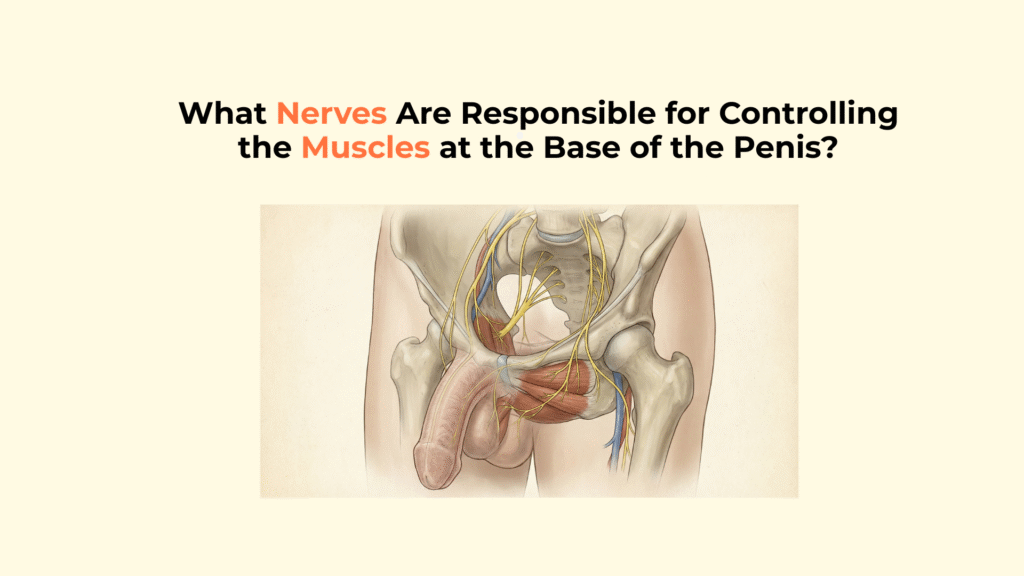
What Nerves Are Responsible for Controlling the Muscles at the Base of the Penis?
The nerves responsible for controlling the muscles at the base of the penis are branches of the Pudendal Nerve—specifically the Deep Branch of the Perineal Nerve—which provides the somatic (voluntary/reflexive) motor signals that drive the Ischiocavernosus and Bulbospongiosus muscles.
These nerves and muscles control the final, powerful mechanical actions of sexual function: maximizing hardness and semen expulsion. This guide details the specific somatic motor pathway, explaining its role in the “supra-systolic pressure” mechanism of erection and the “urethral pump” mechanism of ejaculation.
Important Medical Disclaimer: This information is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Consult with a qualified healthcare provider regarding any concerns about muscle function or nerve damage.
Key Neural Control Facts
- The Nerve: The Pudendal Nerve (via its Perineal branch) provides the motor output.
- The Muscles: Targets are the Ischiocavernosus (rigidity) and Bulbospongiosus (ejaculation).
- The System: This is Somatic control (voluntary/reflexive), distinct from the Autonomic nerves that control blood flow.
- The Rigidity Role: Ischiocavernosus contraction creates supra-systolic pressure (pressure above blood pressure) for maximum hardness.
- The Expulsion Role: Bulbospongiosus contracts rhythmically to expel semen (the “urethral pump”).
What Is the Origin and Primary Function of the Nerves Controlling the Base Muscles?
The nerves controlling the base muscles originate from the Pudendal Nerve in the sacral spine, providing the somatic motor output necessary for these striated muscles to function.
The Somatic Motor Control Hub
The control hub for these powerful pelvic muscles is the Pudendal Nerve, with its Deep Branch of the Perineal Nerve providing the specific voluntary motor innervation. This somatic control allows for both reflexive contractions (during ejaculation) and voluntary engagement (e.g., during Kegel exercises).
Although the Perineal branch of the Pudendal nerve provides direct motor control to the base muscles, sensory feedback during stimulation is transmitted independently through the dorsal nerve of the penis, allowing tactile input to modulate reflexive contraction intensity.
The Target Muscles
The Perineal Nerve targets the two key pairs of striated muscles that cover the root of the penis: the Ischiocavernosus and the Bulbospongiosus.
- Ischiocavernosus: Paired muscles covering the crura (roots) of the penis.
- Bulbospongiosus: Encircles the bulb of the corpus spongiosum and the proximal urethra.
How Do These Nerves Control the Ischiocavernosus Muscle for Rigidity?
The nerves control the Ischiocavernosus muscle for rigidity through the powerful “Supra-Systolic Pressure” Mechanism, which enhances the erection hardness beyond what blood flow alone can achieve.
The “Supra-Systolic Pressure” Mechanism
The Perineal Nerve fires rhythmically, causing the Ischiocavernosus muscle to contract forcefully. This contraction compresses the base of the corpora cavernosa (crura) against the pubic arch.
The force generated by Ischiocavernosus contraction is applied directly against the bony framework anchoring the root of the penis, converting muscular shortening into crural compression and pressure amplification. These compressive forces act specifically on the crura of the corpora cavernosa, preventing venous escape at the origin of the erectile cylinders.
The sustained contraction prevents venous outflow from the crura, boosting the internal pressure to levels above systemic systolic pressure (supra-systolic), which is the final stage of achieving ‘rock-hard’ erection. Venous resistance created by this muscular clamp is transmitted downstream into the cavernosal venous drainage system, delaying outflow and stabilizing intracavernosal pressure during peak rigidity.
The amplified pressure generated by somatic contraction is mechanically contained by the tensile resistance of the tunica albuginea, preventing over-expansion and venous collapse. This contraction can raise intracavernosal pressure to 150 mmHg or more (Source).
How Do These Nerves Control the Bulbospongiosus Muscle for Ejaculation?
The Bulbospongiosus muscle is controlled by the Pudendal Nerve to execute the “Urethral Pump” Mechanism, which is essential for the forceful expulsion of semen.
The “Urethral Pump” Mechanism
During orgasm, the Perineal Nerve sends rapid, strong motor signals that cause the Bulbospongiosus muscle to contract rhythmically. This muscle contraction effectively “milks” the urethra, forcefully expelling semen during the ejaculatory phase.
Secondary Role in Detumescence
The rhythmic contraction of the Bulbospongiosus muscle also has a secondary role in detumescence (going flaccid). Contraction helps expel the last residual venous blood from the corpus spongiosum and cavernosum, aiding in the return to the flaccid state.
Comparative Matrix: Base Muscle Control vs. Erectile Control
This comparison matrix highlights the neurological division of labor for male sexual function.
While the base muscles elevate rigidity mechanically, blood inflow itself is governed by involuntary autonomic signaling described in autonomic penile blood-flow regulation, highlighting the dual-system architecture of erection.
| Function | Nerves | System | Target Tissue |
|---|---|---|---|
| Rigidity / Ejaculation Expulsion | Deep Perineal / Pudendal | Somatic / Voluntary | Striated Muscle (Ischiocavernosus/Bulbospongiosus) |
| Blood Flow / Vasodilation | Cavernous Nerves | Autonomic / Involuntary | Smooth Muscle / Arteries |
| Blood Flow / Vasoconstriction | Cavernous Nerves | Autonomic / Involuntary | Smooth Muscle / Arteries |
What Are the Clinical Implications of Base Muscle Nerve Control?
The clear neurological control of the base muscles is utilized clinically for diagnostic testing and pelvic floor rehabilitation. When asymmetric fibrosis disrupts this closed pressure system, curvature disorders such as Peyronie’s disease may interfere with both corporal expansion and base-muscle efficiency.
The Bulbocavernosus Reflex (BCR) Test
The Bulbocavernosus Reflex (BCR) is a clinical test used to check the integrity of the Pudendal Nerve motor pathway and the S2-S4 spinal cord segment.
Absence of the reflex confirms a compromise to the Pudendal Nerve motor pathway. (Source)
Pelvic Floor Rehabilitation
Exercises like Kegels directly target the Bulbospongiosus and Ischiocavernosus muscles to improve male sexual function.
Rehabilitation efforts focus on improving both urinary continence and the force/rigidity of erection, confirming the somatic system’s role.
Identifying the Base Muscle Control Mechanism
Use this checklist to review the key functional roles of the nerves controlling the penis base.
- ✓ Primary Nerve: Is the Pudendal Nerve (via the Perineal branch) identified as the source?
- ✓ Muscle Targets: Are the Ischiocavernosus and Bulbospongiosus listed?
- ✓ Rigidity Role: Is Ischiocavernosus linked to supra-systolic pressure?
- ✓ Ejaculation Role: Is Bulbospongiosus linked to semen expulsion?
- ✓ System: Is the control explicitly labeled as Somatic (voluntary/reflexive)?
Glossary of Motor & Reflex Terms
To ensure full clarity, this glossary defines the key neuro-muscular terms used throughout this guide.
- Pudendal Nerve
- The major nerve of the pelvis that provides motor control to the muscles of the perineum.
- Ischiocavernosus Muscle
- The muscle that covers the crura and contracts to create maximum erectile rigidity.
- Bulbospongiosus Muscle
- The muscle that covers the bulb and contracts rhythmically to expel semen during ejaculation.
- Supra-Systolic Pressure
- Intracavernosal pressure that exceeds the body’s normal blood pressure, achieved by muscle contraction.
- Somatic Nervous System
- The system responsible for voluntary motor control of skeletal muscles.
- Bulbocavernosus Reflex (BCR)
- A spinal reflex test used to check the integrity of the Pudendal Nerve motor pathway.
Conclusion
In conclusion, the striated muscles at the base of the penis are controlled by the somatic division of the Pudendal Nerve, enabling the essential motor functions of supra-systolic rigidity and ejaculation expulsion. This somatic–autonomic synchronization completes the transformation outlined in the flaccid-to-erect blood-flow sequence, where hydraulic filling becomes mechanically locked.
At Factbasedurology, we believe that understanding the muscular-neural link is key to optimizing pelvic health. The ability to achieve and maintain maximum hardness is driven, quite literally, by the power of these pelvic muscles.